Apollonian
Guest Columnist
Mercola: Are the COVID Jabs Responsible for Rising Mortality Trends?
by Dr. Joseph Mercola | Mercola.comOctober 21st 2021, 12:03 pm
Link: https://www.infowars.com/posts/mercola-are-the-covid-jabs-responsible-for-rising-mortality-trends/
Did COVID-19 raise the death toll despite mass vaccination, or are people dying at increased rates because of it?
"Between 800,000 and 2 million so-called 'COVID19 deaths' may in fact be vaccine-induced deaths.”
STORY AT-A-GLANCE
- According to all-cause mortality statistics adjusted for population growth, the number of Americans who have died between January 2021 and August 2021 is 14% higher than 2018, the pre-COVID year with the highest all-cause mortality, and 16% higher than the average death rate between 2015 and 2019
- Did COVID-19 raise the death toll despite mass vaccination, or are people dying at increased rates because of it?
- The COVID jab killed an estimated 1,018 people per million doses administered during the first 30 days of the European vaccination campaign
- When counting only deaths categorized as COVID-19 deaths, the death toll from the jabs is estimated to be between 200 and 500 deaths per million doses administered. With 4 billion doses having been administered around the world, that means 800,000 to 2 million so-called “COVID-19 deaths” may in fact be vaccine-induced deaths
- Data from 23 countries reveal the number of new COVID cases (i.e., positive tests) after the start of the COVID jab campaign is 3.8 times higher than it was before the rollout of the shots, and the daily COVID death rate is 3.82 times higher

The obvious question is, why did more people die in 2021 (January through August) despite the rollout of COVID shots in December 2020? Did COVID-19 raise the death toll despite mass vaccination, or are people dying at increased rates because of the COVID jabs?
Vaccine-Induced Mortality
In a two-part series,2 Matthew Crawford of the Rounding the Earth Newsletter, examined mortality statistics before and after the rollout of the COVID shots. In Part 1,3 he revealed the shots killed an estimated 1,018 people per million doses administered (note, this is doses, not the number of individuals vaccinated) during the first 30 days of the European vaccination campaign.After adjusting for deaths categorized as COVID-19 deaths, he came up with an estimate of 200 to 500 deaths per million doses administered. With 4 billion doses having been administered around the world, that means 800,000 to 2 million so-called “COVID-19 deaths” may in fact be vaccine-induced deaths. As explained by Crawford:4“Between 800,000 and 2 million so-called ‘COVID19 deaths’ may in fact be vaccine-induced deaths.”
“This does not even include vaccine-induced deaths that have not been recorded as COVID cases, though I suspect that latter number is smaller since the only good way to hide the vaccine mortality signal is to smuggle deaths through the already-established COVID death toll.”
Corroborating Crawford’s calculations are data from Norway, where 23 deaths were reported following the COVID jab at a time when only 40,000 Norwegians had received the shot.

Not taking into account the possibility of underreporting in Norway, that gives us a mortality rate of 575 deaths per million doses administered. What’s more, after conducting autopsies on 13 of those deaths, all 13 were determined to be linked to the COVID jab. As reported by Norway Today back in January 2021:5
“‘The reports might indicate that common side effects from mRNA vaccines, such as fever and nausea, may have led to deaths in some frail patients,’ chief physician Sigurd Hortemo in the Norwegian Medicines Agency noted.
The Norwegian Medicines Agency and the National Institute of Public Health (FHI) jointly assess all side effects reports. As a result, the FHI has updated the corona vaccination guide with new advice on the vaccination of frail elderly people.
‘If you are very frail, you should probably not be vaccinated,’ Steinar Madsen at the Norwegian Medicines Agency said at a webinar on corona vaccine for journalists …”
Is the COVID Jab Responsible for Excess Deaths?
Crawford goes on to look at data from countries that have substantial vaccine uptake while simultaneously having very low rates of COVID-19. This way, you can get a better idea as to whether the COVID jabs might be responsible for the excess deaths, as opposed to the infection itself.He identified 23 countries that fit this criteria, accounting for 1.88 billion individuals, roughly one-quarter of the global population. Before the COVID jabs rolled out, these nations reported a total of 103.2 COVID-related deaths per million residents. Five nations had more than 200 COVID deaths per million while seven had fewer than 10 deaths per million.
As of August 1, 2021, 25.35% of inhabitants in these 23 nations had received a COVID jab and 10.36% were considered fully vaccinated. In all, 673 million doses had been administered. Based on these data, Crawford estimates the excess death rate per million vaccine doses is 411, well within the window of the 200 to 500 range he calculated in Part 1.
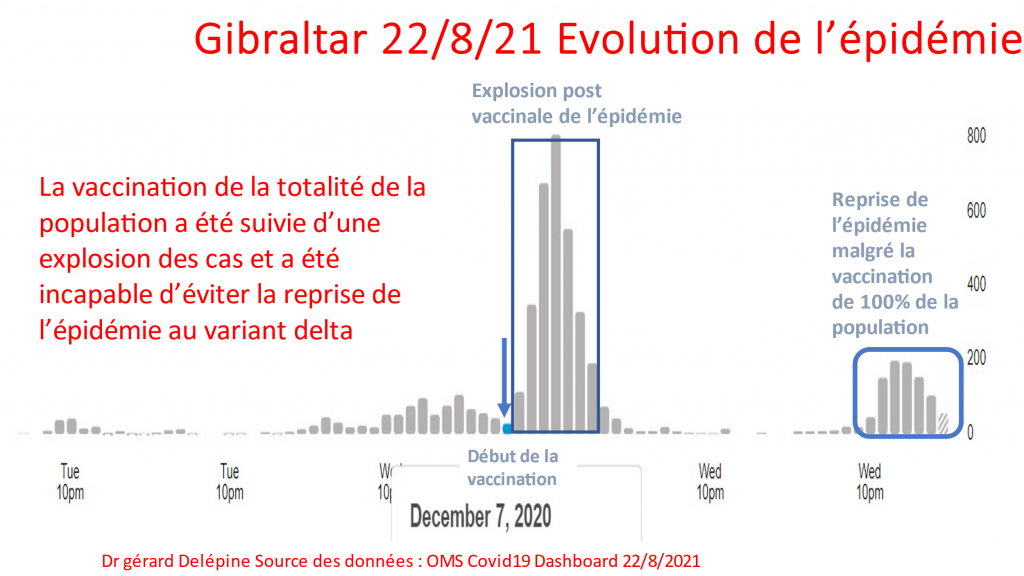
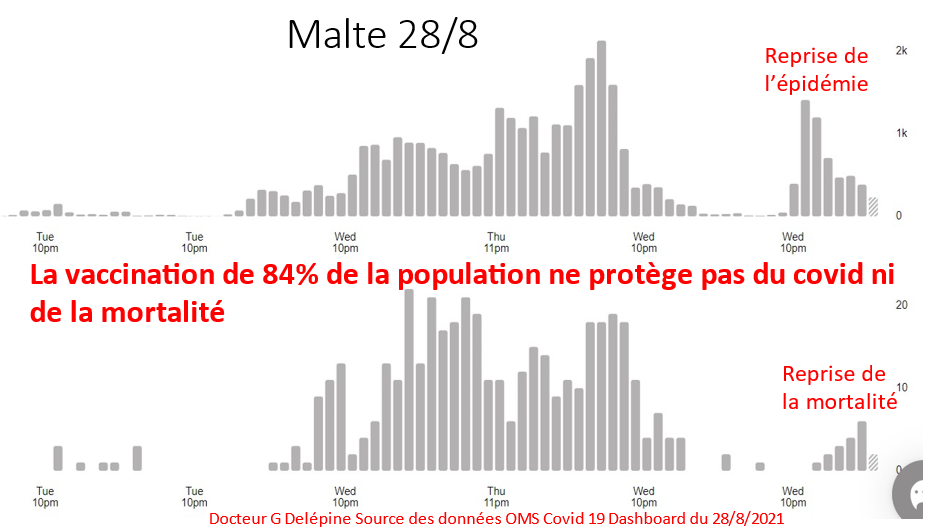
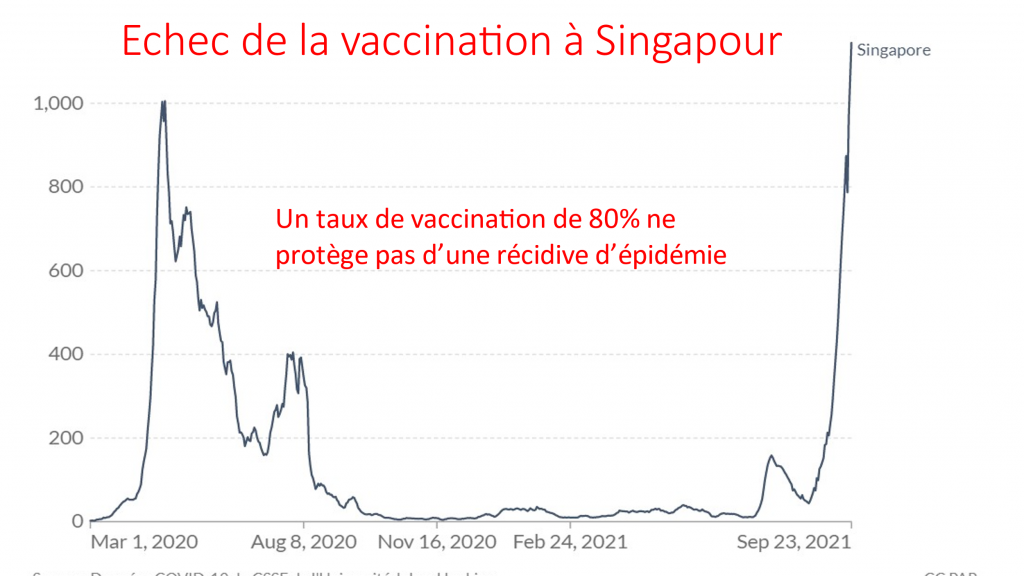
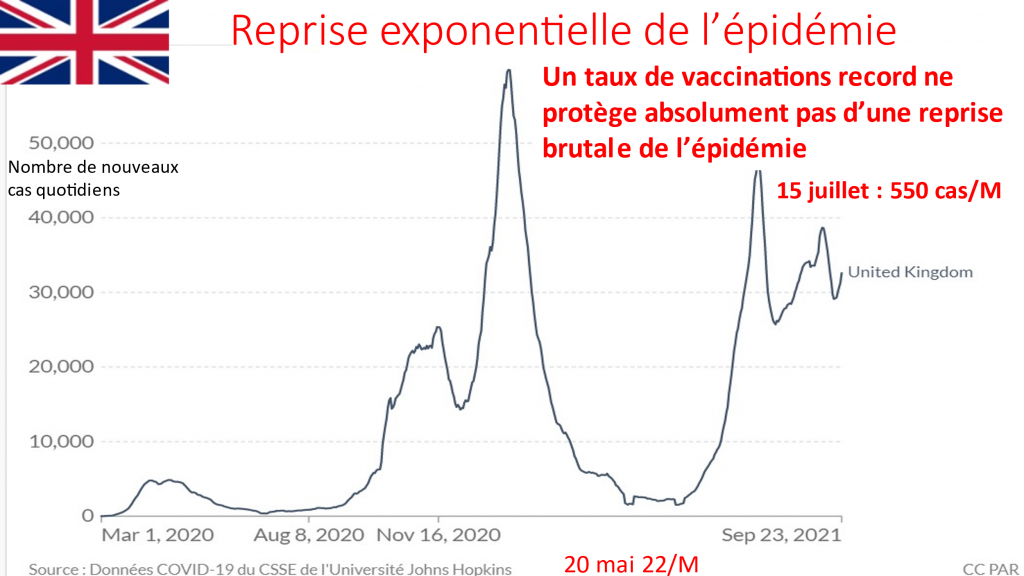
Equally intriguing is the finding that the number of new COVID cases (i.e., positive tests) after the start of the COVID jab campaign is 3.8 times higher than it was before the rollout of the shots, and the daily COVID death rate is 3.82 times higher.
Morocco and Saudi Arabia were the only two nations in which the case rate and COVID death rates went down after the vaccination campaign started. “If deaths were scaled by 3.82 due to the vaccines, then there were 276,465 excess deaths during this time span,” Crawford writes.
He goes through a number of adjustments to remove outliers that might skew the data sets, so for a more detailed review, see the original article. But in summary, after removing nations with more than 100 COVID deaths per million before their vaccination program (to evaluate the impact of the shots alone), he came up with 13 countries with a combined population of 354 million.
The number of doses administered in these 13 countries is similar to the original cohort. The adjusted number of excess deaths per million is now 318, which is still within the 200 to 500 per million range.
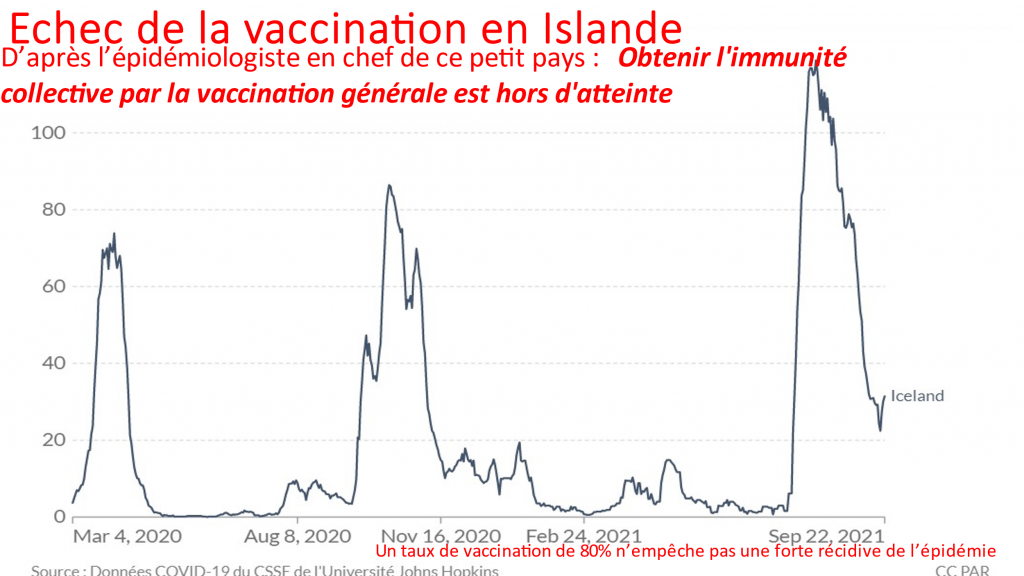
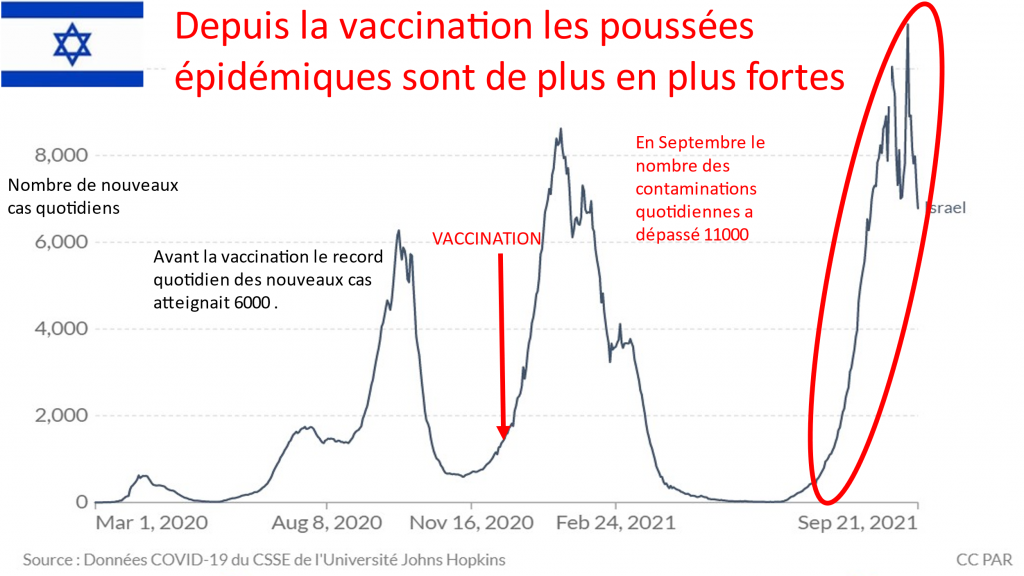
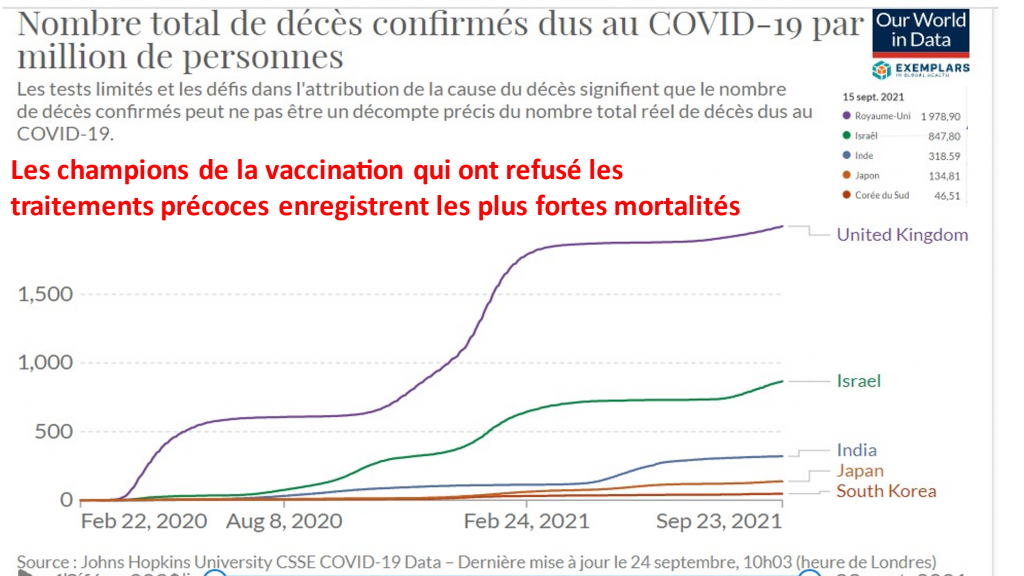
Remarkably, though, the number of COVID deaths in these 13 countries is 11.61 times higher post-vaccination, compared to before the jabs were rolled out. In five of the 13 countries, a whopping 90% of their COVID-19 fatalities have been logged after their vaccination campaigns began! This obliterates any fantasy that the COVID injections are actually helping.
“On face, these results reinforce the case that the experimental vaccines are killing people,” Crawford writes. “At the very least, this is one more dramatic [lack of] safety signal that should spur authorities who care about our health to come to the table for a discussion about how to refine the data they’re not analyzing to anyone’s knowledge …
More concerning is that numerous of these nations — largely located in Asia — seemed to have no susceptibility at all to the pandemic prior to vaccination. There are a lot of theories as to why this might be aside from just vaccines triggering deaths.
- Might PCR testing pick up signals from attenuated virus vaccines, resulting in case explosions (from almost none) to match the [new] deaths?
- Could some of these vaccines have faulty production … during polio vaccine rollout? This could result in cases and deaths?
- Paraguay has by far the greatest signal of vaccine-induced mortality. It stands out as one of the only nations on Earth to use both Chinese and also Western vaccines. Is there any reason such a combination could result in more volatile disease spread?
- Do we really believe that the braintrust at the FDA and CDC are entirely unaware of these observations?
US Whistleblower Highlights Underreporting
In mid-July 2021, America’s Frontline Doctors, represented by Renz Law,6 filed a lawsuit7 against the secretary of the U.S. Department of Health and Human Services, Xavier Becerra. In that lawsuit, they cite whistleblower testimony by a computer programmer with expertise in health care data analytics and access to Medicare and Medicaid data maintained by the Centers for Medicare and Medicaid Services (CMS).According to this whistleblower, the U.S. Vaccine Adverse Event Reporting System (VAERS) under-reports deaths caused by the COVID shots by a conservative factor of five or more. She claims the number of Americans killed by the shots was at least 45,000 as of July 9, 2021.
At that time, VAERS reported 9,048 deaths following COVID injection. That number is now 16,310 (as of October 1, 20218). Using an under-reporting factor of five, that gives us an estimated death toll of 81,550.
COVID Shots May Have Killed More Than 200,000 in the US
Steve Kirsch, executive director of the COVID-19 Early Treatment Fund, has come up with even more drastic numbers. In the video “Vaccine Secrets: COVID Crisis,”9 he argues that VAERS can be used to determine causality, and shows how the VAERS data indicate more than 212,000 Americans have already been killed by the COVID shots.10Anywhere from 2 million to 5 million have also been injured by them in some way. Kirsch is so confident in his analyses, he’s offered a $1 million academic grant to anyone who can show his analysis is flawed by a factor of four or more. He’s even offered $1 million to any official willing to simply have a public debate with him about the data, and none has accepted the challenge.
Woman’s Obituary Blames COVID Vaccine for Her Death
While it may be challenging to determine exactly how many people have died as a direct result of the COVID shots, we can be certain that deaths are occurring.One Oregon woman’s obituary11 went viral after her family blamed side effects of the COVID-19 vaccine on her death. The family minced no words, calling out state and local governments for their “heavy-handed vaccine mandates.” Jessica Berg Wilson left behind a husband and two young daughters, aged 5 and 3.
“Jessica Berg Wilson, 37, of Seattle, Washington, passed away unexpectedly September 7, 2021 from COVID-19 vaccine-induced thrombotic thrombocytopenia (VITT) surrounded by her loving family,” the obituary states.12
“Jessica was an exceptionally healthy and vibrant 37-year-old young mother with no underlying health conditions … Local and state governments were determined to strip away her right to consult her wisdom and enjoy her freedom.
She had been vehemently opposed to taking the vaccine, knowing she was in good health and of a young age and thus not at risk for serious illness. In her mind, the known and unknown risks of the unproven vaccine were more of a threat.
But, slowly, day by day, her freedom to choose was stripped away. Her passion to be actively involved in her children’s education — which included being a Room Mom — was, once again, blocked by government mandate.
Ultimately, those who closed doors and separated mothers from their children prevailed. It cost Jessica her life. It cost her children the loving embrace of their caring mother. And it cost her husband the sacred love of his devoted wife.”
COVID Jab Effects Are Rapidly Waning
To add insult to injury, there’s ample evidence showing that whatever benefit you glean from the COVID jab is short-lived, requiring you to risk life and limb yet again with another booster shot (and probably more to come after that).If you need a refresher on the potential mechanisms of harm, download and read Stephanie Seneff’s excellent paper,13 “Worse Than The Disease: Reviewing Some Possible Unintended Consequences of mRNA Vaccines Against COVID-19,” published in the International Journal of Vaccine Theory, Practice and Research in collaboration with Dr. Greg Nigh.
Among those incriminating data sets is an analysis by Humetrix,14 which assessed the effectiveness of mRNA COVID-19 vaccines against the delta variant among 5.6 million Medicare beneficiaries, aged 65 and older. Three key questions answered by the data analysis are:
- Is vaccine effectiveness waning over time?
- Is vaccine effectiveness reduced for the delta variant?
- Does the need for a booster shot vary by sub-population?
- Yes, the effectiveness of both Moderna and Pfizer’s injections rapidly wane in this cohort.
- As of mid-August 2021, the vaccine effectiveness against delta infection was only 41% and effectiveness against hospitalization due to the delta variant was 62%, both of which are “lower than previously reported.”
- The shots were even less effective in those over the age of 75, and a breakthrough hospitalization risk model suggests prioritizing people over age 65 for boosters.
Breakthrough Infections Don’t Seem so Rare in the Elderly
According to Humetrix, between January 2021 and August 14, 2021, 5.6 million Medicare beneficiaries (out of 20 million) were fully vaccinated with either two doses of Pfizer or Moderna, or one dose of Janssen.Of those, 148,000 experienced a breakthrough infection, 30,000 required hospitalization and 9,400 needed intensive care. That means breakthrough infections in this age group occur at a rate of about 1 in 38, which doesn’t strike me as being particularly rare.
As per Centers for Disease Control and Prevention guidance, patients were only considered fully vaccinated two weeks after the second dose. So, anyone who developed COVID-19 symptoms before then were not counted.
While the analysis reports success, saying the hospitalization rate for breakthrough infections was reduced by one-third compared to the hospitalization rate between March and December 2020, and the death rate in breakthrough infections was reduced six-fold, a central problem remains.
The shots don’t protect you for very long. As shown on Page 8 of the PowerPoint, the breakthrough infection rate at five and six months’ post-vaccination is double the rate at three and four months’ post-vaccination.
Considering the risk of lethal vaccine injury is elevated in the elderly — as noted by the Norwegian Medicines Agency — starting them on a treadmill of booster shots strikes me as an idea that can only end in heartbreak for families around the world.
“The Truth About COVID-19” exposes the hidden agenda behind the pandemic, showing the countermeasures have nothing to do with public health and everything to do with ushering in a new social and economic system based on totalitarian, technocracy-led control. So, it’s not misinformation they fear. It’s the truth they want to prevent from spreading. Pick up a copy of this best-selling book today before it’s too late.
- 1 Twitter Jeremy Horpedahl October 7, 2021
- 2, 4 Rounding the Earth Newsletter August 7, 2021
- 3 Rounding the Earth Newsletter August 5, 2021
- 5 Norway Today January 14, 2021
- 6 Renz-law.com
- 7 US District Court for the Northern District of Alabama Civil Action No: 2: 21-cv-00702-CLM (PDF)
- 8 OpenVAERS Data as of October 1, 2021
- 9 Lew Rockwell October 11, 2021
- 10 SKirsch.io/vaccine-resources
- 11, 12 Obits.Oregonlive.com Jessica Berg Wilson
- 13 International Journal of Vaccine Theory, Practice and Research May 10, 2021; 2(1): 38-79
- 14 Humetrix Powerpoint September 21, 2021